

Abstract
Background
In USA in 2007, it was estimated that approximately one third of hospitalized patients, approximately 12 million patients per year receive heparin. Heparin induced thrombocytopenia (HIT) is one of the serious complications of Heparin resulting from immune mediated antibody.
4Ts score is the imperative tool to help differentiate HIT from other causes of thrombocytopenia. The 4Ts score decreases not only risk of bleeding by avoiding anticoagulant but also cost of health care by testing only patients with intermediate to high pretest probability.
Our study suggests 4Ts scores calculators are to be introduced as a part of order set for HIT tests.
Objective
This retrospective study is Part III of our prior studies " Are We Doing Too Many HIT tests", to decrease false positive HIT patients by improving use and awareness about high negative predictive value of 4T score among physicians. This study was carried out to determine outcomes of our previous study of this series in order to assess the reduction of unnecessary ELISA test orders to diagnose HIT in a single urban community hospital in Chicago.
Method
A retrospective chart review of medical records of the patients (n=181) who underwent H-PF4-ELISA for HIT screening from January 1st, 2016 to December 31st 2017 was conducted.
Data was collected from patient's charts which included the requesting department (i.e. ICU, ED, Medical and surgical floors). Also, date of admission, date of onset of platelet drop, degree of thrombocytopenia, incidence of DVT, PE, arterial thrombosis and bleeding and alternative reasons of platelet count drop other than HIT were collected. For each patient a for calculation of Pretest probability by the 4T score was conducted.
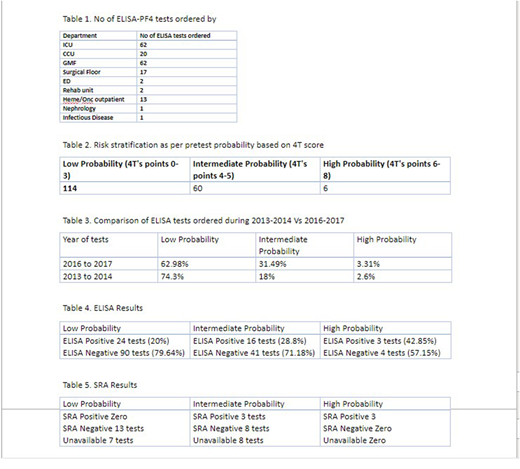
We stratified these patients based on 4Ts score (0-3) for low probability, (4-5) intermediate probability and (6-8) high probability risk for HIT.
We reviewed all charts for which both ELISA and SRA were ordered. Pharmacy department and Hematology labs were contacted to calculate costs of ELISA, SRA and anticoagulation.
Results
Our results showed that 114 (62.98%) of 181 ELISA tests ordered had low pretest probability for HIT. None of these records were found to be true positive by SRA. However, 24(20%) of low probability category were found positive by ELISA and received anticoagulation and thus were exposed to higher risk of bleeding and additional health care costs.
There were 57 (31.49%) out of 181 records had intermediate probability. 16 patients with intermediate probability were ELISA test positive. However, 3 (5.26%) of intermediate probability patients were found to be true positive by SRA.
While only 6 (3.31%) out of 181 patients records had high probability for HIT and 3 patients (50%) of high probability were found to be true positive by SRA.
However, 11 patients from low probability category and 5 patients from intermediate probability category did not have SRA results in their medical record.
Discussion
In our previous study, 74.3% of patients tested for HIT during Jan.2013 to Dec. 2014were found to have low probability compared to 62.98% of our current study.
Interestingly, patients with intermediate probability have increased to 31.49% from 18% from our previous study. This is a desired decreased.
Cost for ELISA test for HIT ranges $200 to $300 per test and cost of SRA is roughly $50 to $60. Cost of one day of Argatroban treatment is roughly $670 which brings the total cost per patient roughly $1000 per day for all those patients who are tested positive by ELISA.
34,200 USD were spent on ELISA test for 114 patients with low probability 4T score who were found true negative.
Furthermore, 20 patients with false positive ELISA from low probability 4T category were exposed to 40,200 USD worth of Argatroban during three days while SRA results were awaited.
As per our study, educational interventions in our hospital have made remarkable improvement in decreasing the number of ELISA test in patients with low pretest probability from 74.3% to 62.98%
Lastly, more than 74,000 USD per 114 patients (with low probability score) could be reduced by introducing "4T score calculation Alert" as a part of order set for HIT in EMR software.
We conclude that incorporating prescreening for HIT with 4T score calculation as a part of order set for ELISA could decrease not only the risk of bleeding but also avoidable additional health care cost.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal